Atrial fibrillation
Page highlights:
How many Australians have atrial fibrillation?
- Atrial fibrillation affects approximately 2.2% of the general population – equivalent to more than 500,000 people in 2021.
- In 2020–21, there were around 201,000 hospitalisations where atrial fibrillation recorded as the principal and/or additional diagnosis.
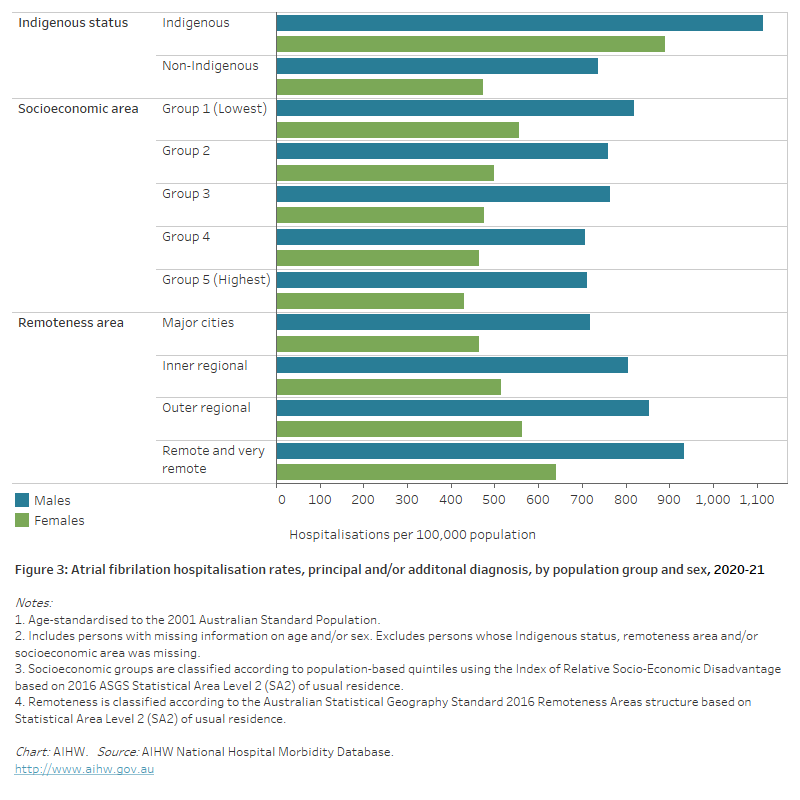
In 2020–21, atrial fibrillation hospitalisation rates were 21% higher for people living in the lowest socioeconomic areas compared with those in the highest socioeconomic areas.
 Atrial fibrillation contributed to 16,300 deaths (9.5% of all deaths) in 2021.
Atrial fibrillation contributed to 16,300 deaths (9.5% of all deaths) in 2021.
What is atrial fibrillation?
Atrial fibrillation (AF) is a disturbance of the electrical system of the heart, where the heart beats with an abnormal rhythm, and does not pump blood regularly or work as efficiently as it should.
Often, people with AF do not know that they have it, and they do not experience any symptoms. Others may experience an irregular pulse, heart palpitations (‘fluttering’), fatigue, weakness, discomfort, shortness of breath or dizziness.
Common causes of AF include long-term high blood pressure, coronary heart disease and valvular heart disease. For some people, there is no apparent cause.
The risk of developing AF is higher in older people. Other risks include obesity, diabetes, CKD, obstructive sleep apnoea, smoking and alcohol consumption above guideline levels.
AF increases the risk of stroke, and strokes associated with AF are more severe with a risk of death twice that of other stroke causes. An individual’s risk may be even higher if their AF is associated with previous heart disease or with other chronic diseases (NHFA 2016).
How many Australians have atrial fibrillation?
Currently, there are no national data sources that report on the total number of Australians living with AF.
Surveys and studies on sections of the Australian population suggest that AF affects approximately 2.2% of the general population – equivalent to more than 500,000 people in 2021 (AIHW 2020).
The proportion affected increases with age. An estimated 5.4% of the Australian population aged 55 and over have AF.
Hospitalisations
Often, AF can be managed through the primary care that is provided by general practitioners, allied health services, community health services and community pharmacy. However, some patients with AF will need admission to hospital for investigation and management, and they may require surgical or therapeutic procedures during the admission.
Note that the hospitalisation data presented here are based on admitted patient episodes of care, which exclude non-admitted emergency department care, but can include multiple events experienced by the same individual.
Atrial fibrillation often occurs alongside other chronic diseases, so both the principal and additional diagnoses of AF should be counted when estimating its contribution to hospitalisations.
There were around 201,000 hospitalisations where AF was recorded as the principal and/or additional diagnosis in 2020–21, at a rate of 785 per 100,000 population. This represents 1.7% of all hospitalisations in Australia.
Atrial fibrillation was recorded as the principal diagnosis in 38% (76,200) of these hospitalisations.
In those cases where AF was listed as an additional diagnosis, common principal diagnoses include other cardiovascular diseases (heart failure, stroke, acute myocardial infarction), pneumonia, sepsis, chronic obstructive pulmonary disease and fracture of femur (AIHW 2020).
Age and sex
Where AF was recorded as the principal and/or additional diagnosis, hospitalisation rates:
- were overall 1.6 times as high for males as females, after adjusting for differences in the age structure of the populations. Age-specific rates were higher among males than females in all age groups
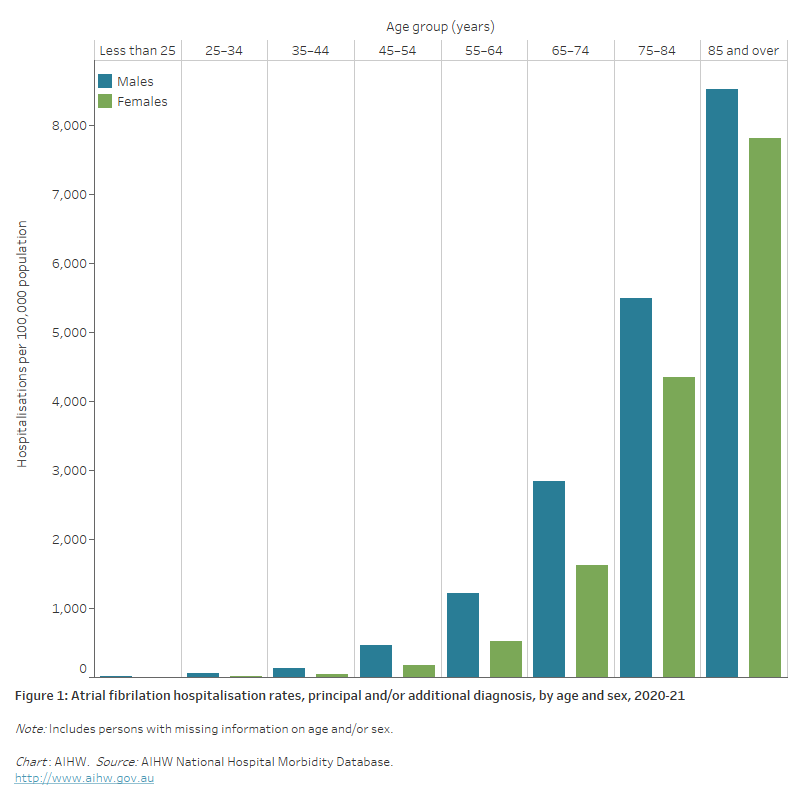
- increased with age, with rates highest for males and females aged 85 and over – at least 1.6 times as high as those aged 75–84 (Figure 1).
Figure 1: Atrial fibrillation hospitalisation rates, principal and/or additional diagnosis, by age and sex, 2020–21
The bar chart shows that atrial fibrillation hospitalisation rates in 2020–21 were highest among males and females 85 years and over (8,500 and 7,800 per 100,000 population, respectively).
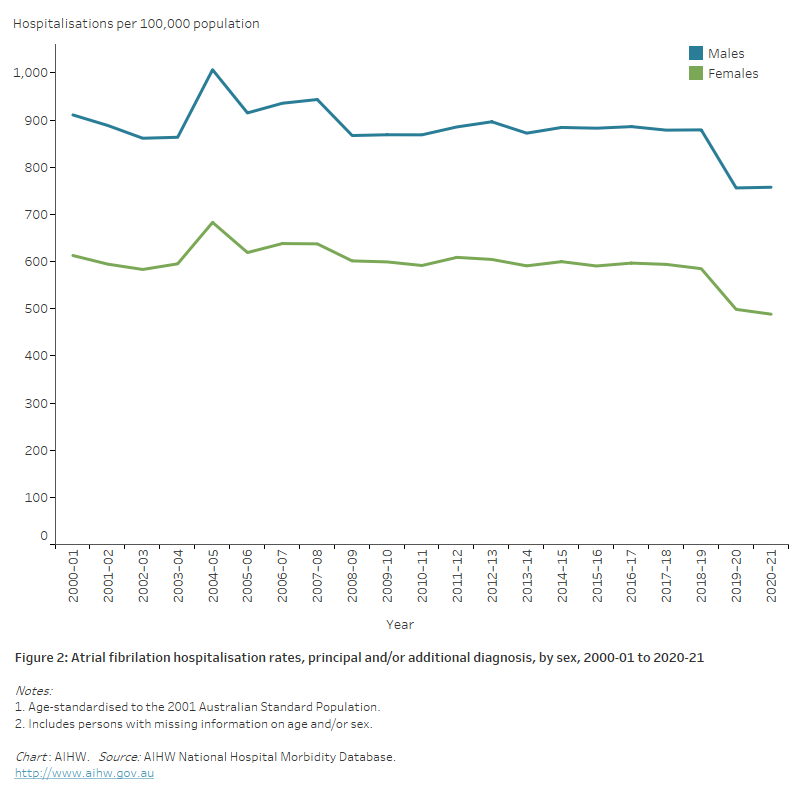
The line chart shows the decline in age-standardised atrial fibrillation hospitalisation rates between 2000–01 and 2020–21 from 911 to 758 per 100,000 population for males and 613 to 488 per 100,000 population for females.
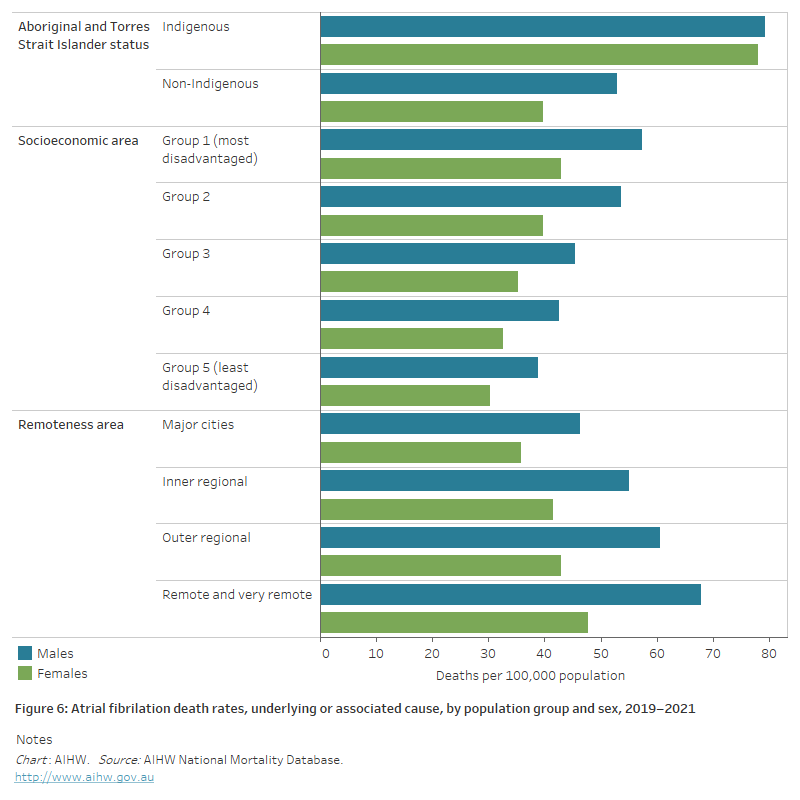
The horizontal bar chart shows that age-standardised atrial fibrillation hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas and people living in Remote and very remote areas.
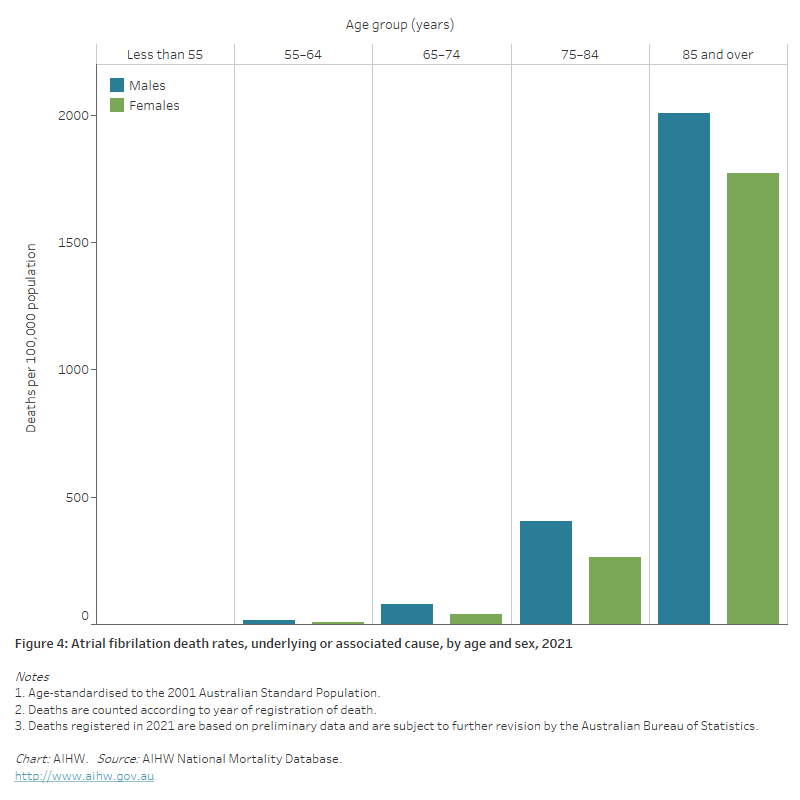
The bar chart shows that atrial fibrillation death rates in 2021 were highest among males and females 85 and over (2,000 and 1,800 per 100,000 population, respectively).
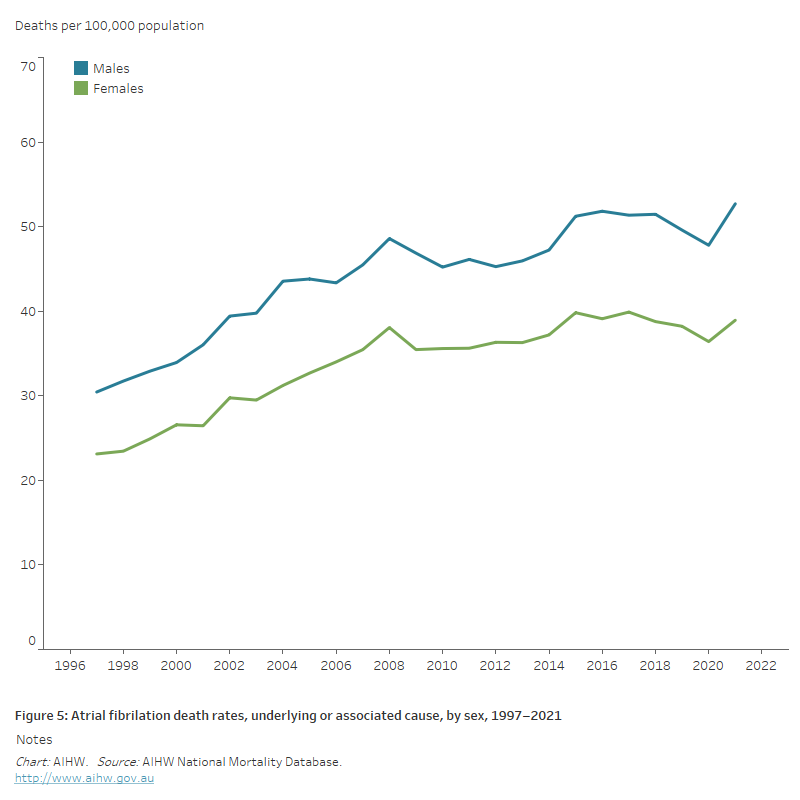
The line chart shows the increase in age-standardised atrial fibrillation death rates between 1997 and 2021 for both males and females, from 30 to 53 and 23 to 39 per 100,000 population, respectively.
The horizontal bar chart shows that age-standardised atrial fibrillation death rates in 2019–2021 were higher among Indigenous Australians, people living in the lowest socioeconomic areas and people living in Remote and very remote areas.