All heart, stroke and vascular disease
Page highlights:
How many Australians have heart, stroke and vascular disease?
- 1.2 million Australians aged 18 and over (6.2% of the adult population) were living with 1 or more conditions related to heart, stroke or vascular disease in 2017–18.
- In 2020–21, there were 600,000 hospitalisations where cardiovascular disease was recorded as the principal diagnosis.
Variation among population groups
- There were around 17,300 hospitalisations with a principal diagnosis of cardiovascular disease among Aboriginal and Torres Strait Islander people in 2020–21.
 In 2021, cardiovascular disease was the underlying cause of 42,700 deaths (25% of all deaths).
In 2021, cardiovascular disease was the underlying cause of 42,700 deaths (25% of all deaths).Between 1980 and 2021 the age-standardised cardiovascular disease death rate declined by around three-quarters.
How many Australians have heart, stroke and vascular disease?
An estimated 1.2 million Australians aged 18 and over (6.2% of the adult population) were living with 1 or more conditions related to heart, stroke or vascular disease, based on self-reported data from the ABS 2017–18 National Health Survey.
Age and sex
In 2017–18, based on self-reported data, the prevalence of heart, stroke and vascular disease among adults:
- was higher among men (641,000, an age-standardised rate of 6.5%) than women (509,000, an age-standardised rate of 4.8%)
- increased with age–more than 1 in 4 (26%) of persons aged 75 and over had heart, stroke and vascular disease (Figure 1).
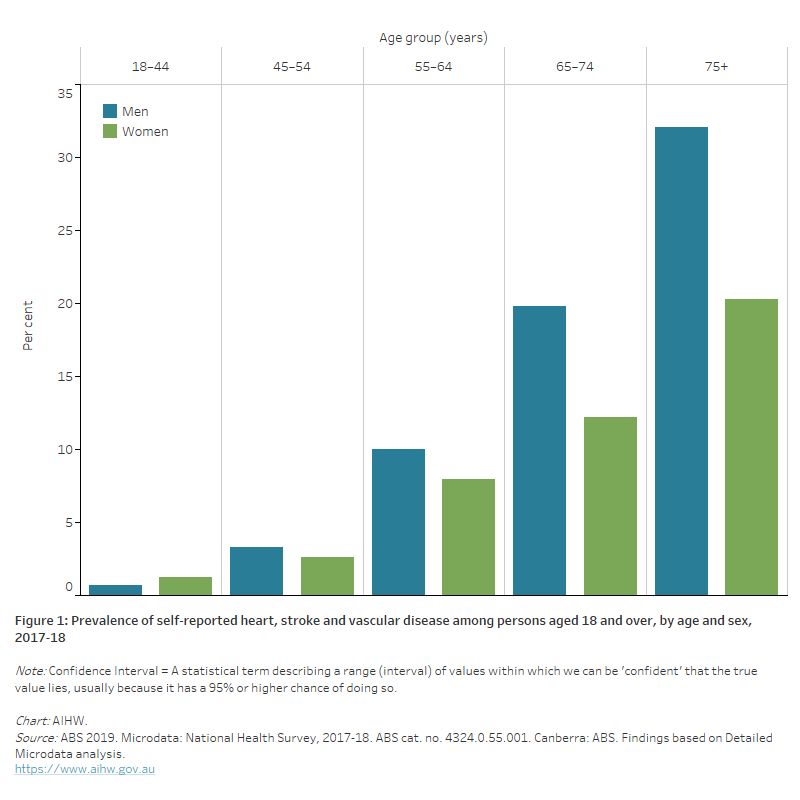
Figure 1: Prevalence of self-reported heart, stroke and vascular disease among persons aged 18 and over, by age and sex, 2017–18.
The bar chart shows the prevalence of self-reported heart, stroke and vascular disease by age group in 2017–18. Rates were highest among men and women aged 75 and over (32% and 20%).
Women and cardiovascular disease
Cardiovascular disease (CVD) is a leading cause of illness and death among Australian women. While more men than women have heart, stroke and vascular disease, the risk in women is largely under-recognised by the population (AIHW 2019). There are aspects of cardiovascular health that are unique among women, with important sex differences in prevention, diagnosis and treatment.
Increased awareness and recognition of these differences will help women avoid under-diagnosis, under-treatment, and under-estimating the risk of dying or becoming seriously unwell due to heart, stroke and vascular disease (World Heart Federation 2021).
More than half a million women have CVD
- Based on self-reported data, an estimated 509,000 (5.4%) women aged 18 and over in Australia had 1 or more heart, stroke and vascular diseases in 2017–18.
A major cause of illness and death
- Around 19,400 women had an acute coronary event (heart attack or unstable angina), and 18,500 women had a stroke in 2020
- 250,000 hospitalisations of women with CVD in 2020–21
- 21,000 women died from CVD in 2021, equivalent to 1 in 4 female deaths.
Indigenous women are disproportionately affected
- Indigenous women were up to twice as likely as non-Indigenous women to have CVD in 2018–19, and to die from coronary heart disease or stroke in 2019–21.
CVD and other chronic conditions are key priorities in the National Women’s Health Strategy 2020–2030 (Department of Health 2019). Increased public awareness and education, investment in research, implementing evidence-based practice, and strategies to address equity issues have been identified as areas for action to improve the heart health of Australian women (Heart Foundation 2021).
For more information:
Cardiovascular disease in Australian women – a snapshot of national statistics, and Cardiovascular disease in women.
 Kylie's story
Kylie's story
‘I always thought that the typical candidate was someone who smoked, sported a beer belly, and had high blood pressure. I was a fit, young, non-smoking woman in my forties. A heart attack couldn’t happen to me – right?'
Kylie survived a heart attack and said cardiac rehab was a turning point in her recovery.
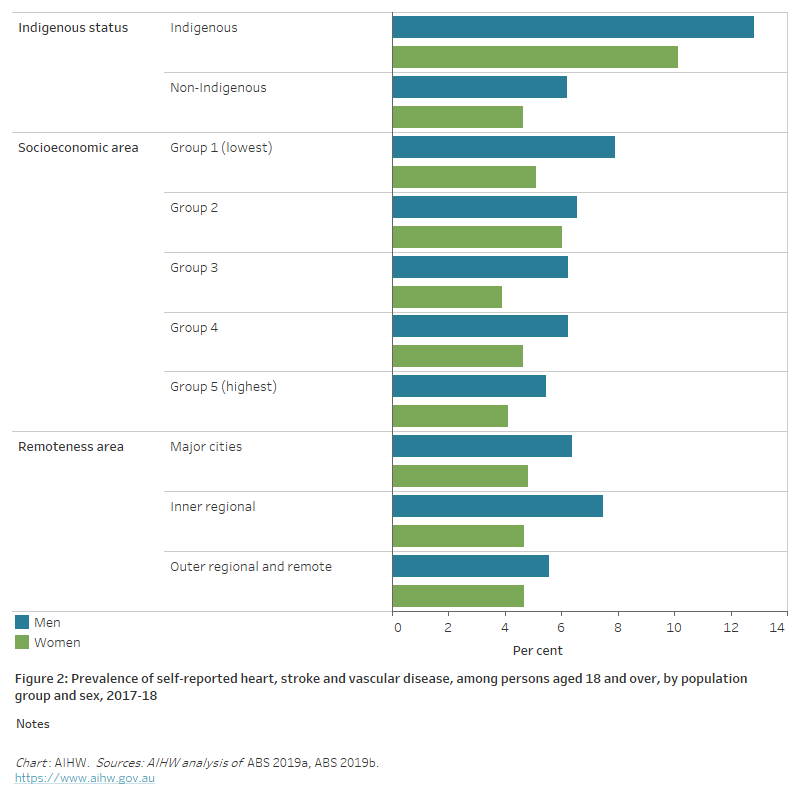
The horizontal bar chart shows that the prevalence of self-reported heart, stroke and vascular disease in 2017–18 was higher among Indigenous Australians, but did not vary significantly by socioeconomic or remoteness areas.
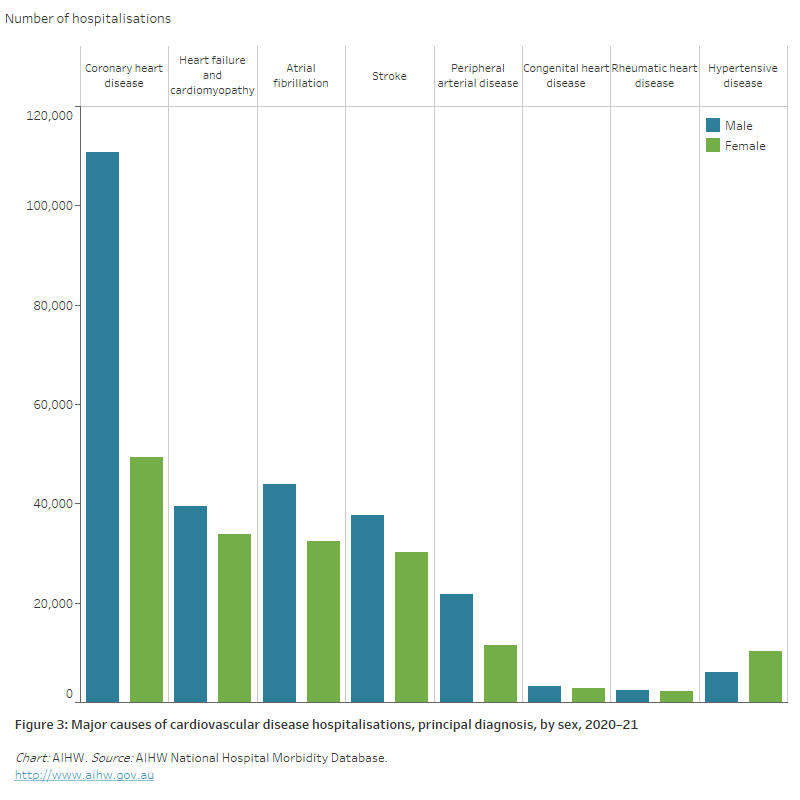
The bar chart shows the number of hospitalisations for selected cardiovascular diseases in 2020–21, ranging from 160,000 for a principal diagnosis of coronary heart disease to 4,600 for rheumatic heart disease.
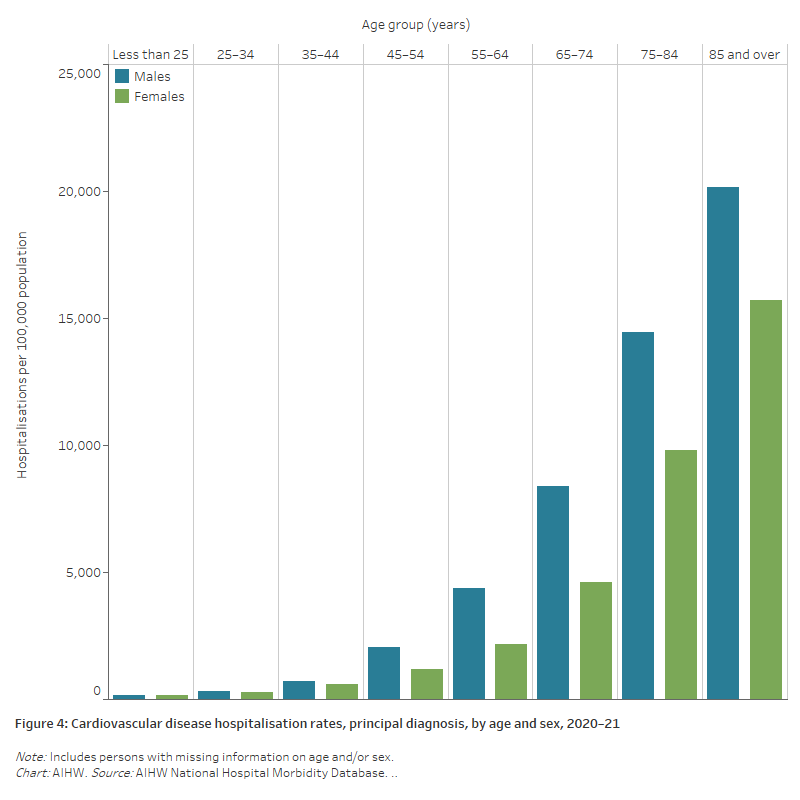
The bar chart shows cardiovascular disease hospitalisation rates by age group in 2020–21. These were highest among men and women aged 85 and over (20,200 and 15,700 per 100,000 population).
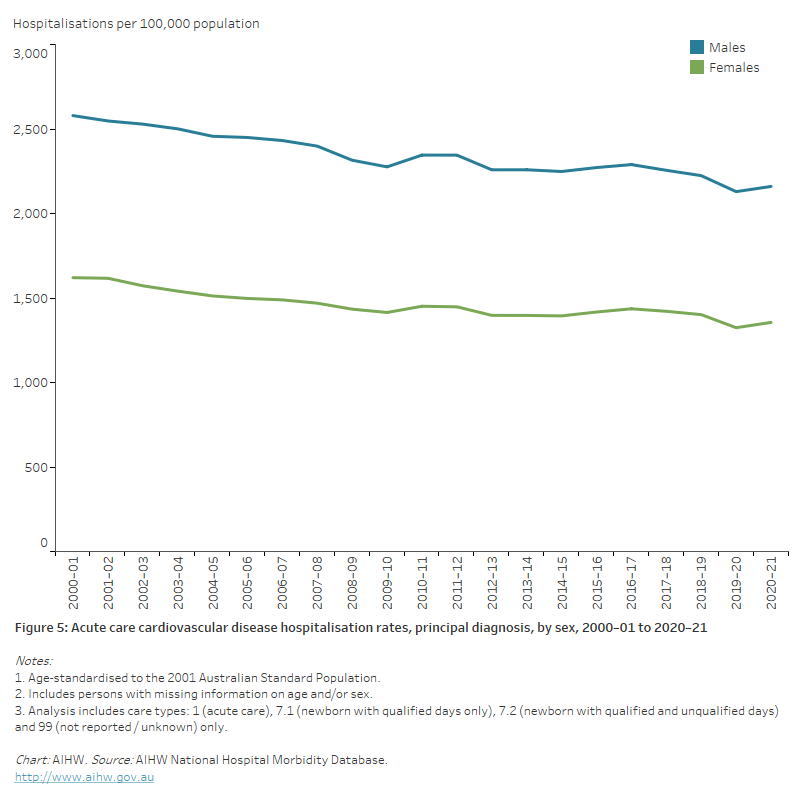
The line chart shows declines in age-standardised rates of male and female acute care CVD hospitalisations between 2000–01 and 2020–21, from 2,570 to 2,160 per 100,000 population for males, and from 1,614 to 1,356 for females.
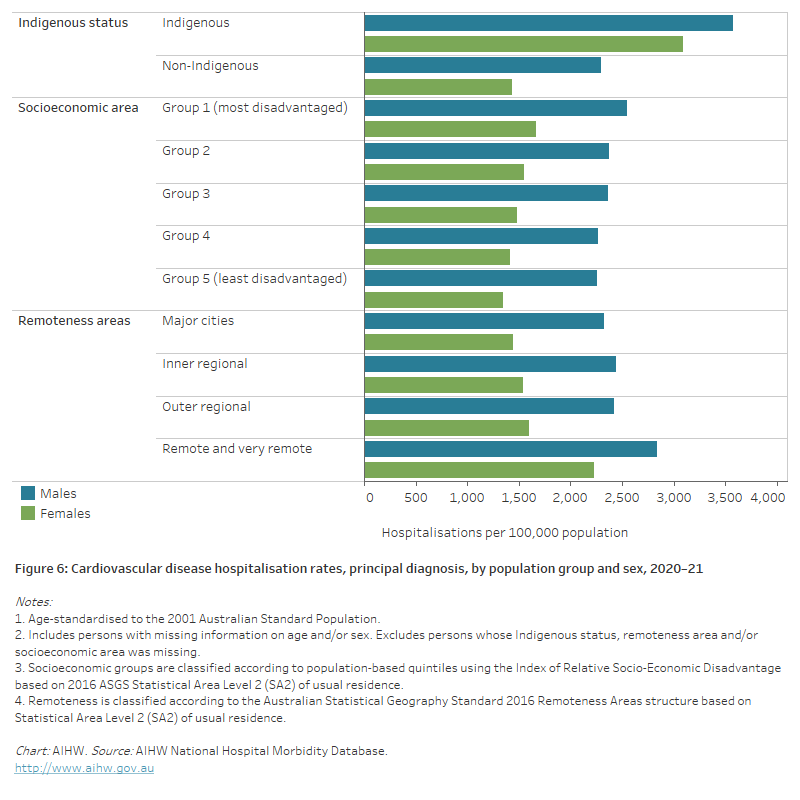
The horizontal bar chart shows that male and female CVD hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.
Deaths
In 2021, CVD was the underlying cause of 42,700 deaths (25% of all deaths), a rate of 166 per 100,000 population.
CVD was the second leading cause of death group in 2021 behind cancers (30% of all deaths), but ahead of diseases of the respiratory system (7.9%), external causes (6.8%), mental and behavioural disorders (6.6%) and diseases of the nervous system (6.5%).
Where CVD was listed as the underlying cause of death in 2021:
- 41% were due to coronary heart disease
- 20% were due to stroke
- 11% were due to heart failure and cardiomyopathy
- 5.7% were due to hypertensive disease
- 5.7% were due to atrial fibrillation
- 4.5% were due to peripheral arterial disease
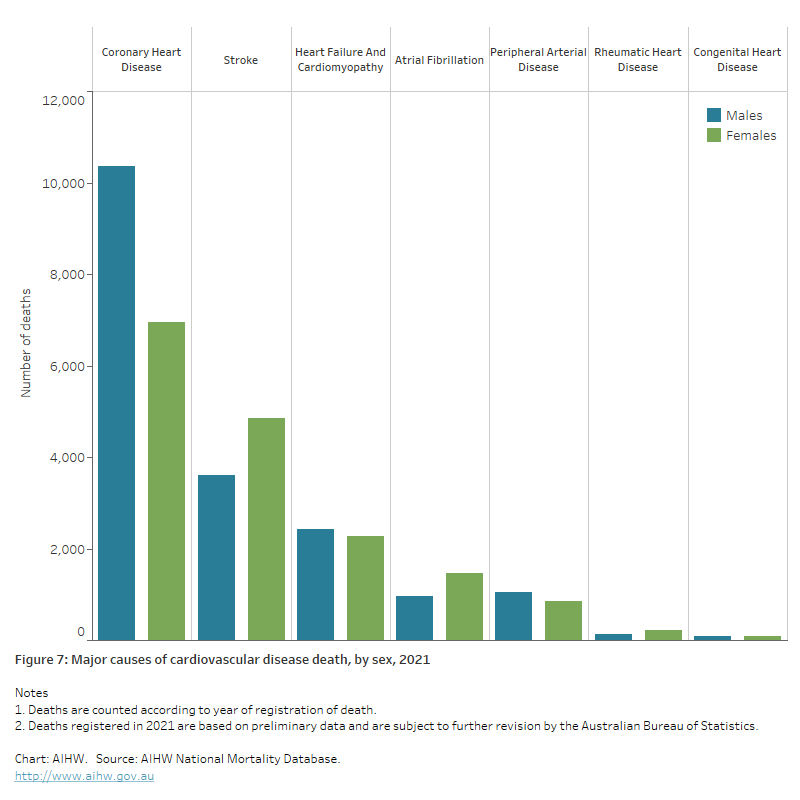
- 0.8% were due to rheumatic heart disease (Figure 7).
Figure 7: Major causes of cardiovascular disease death, 2021
The bar chart shows the number of deaths from selected cardiovascular diseases as an underlying cause in 2021, ranging from 17,300 for coronary heart disease to 340 for rheumatic heart disease.
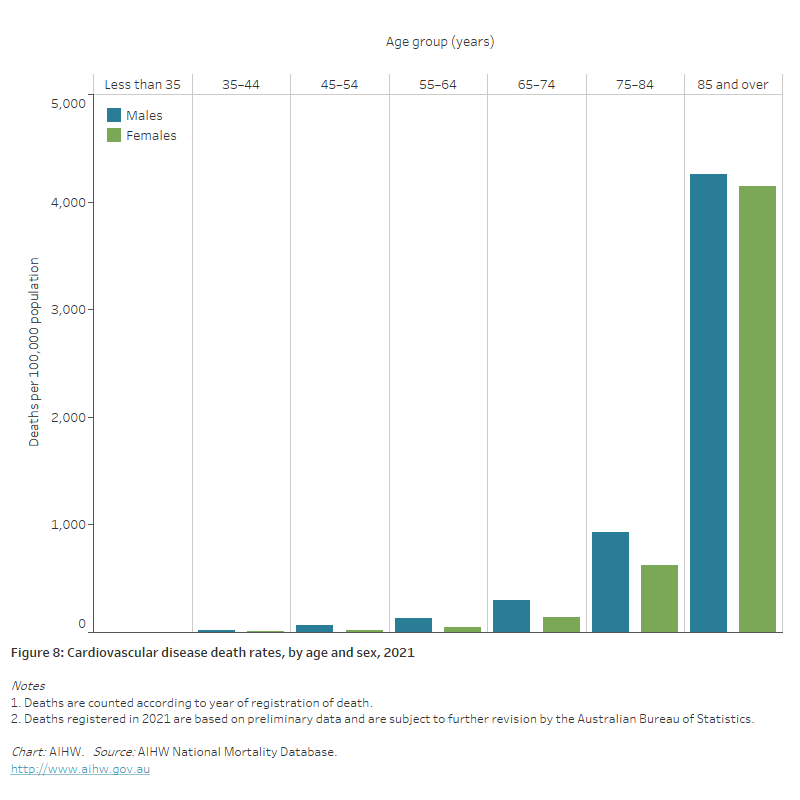
The bar chart shows cardiovascular disease death rates by age group in 2021. These were highest among men and women aged 85 and over (4,300 and 4,100 per 100,000 population).
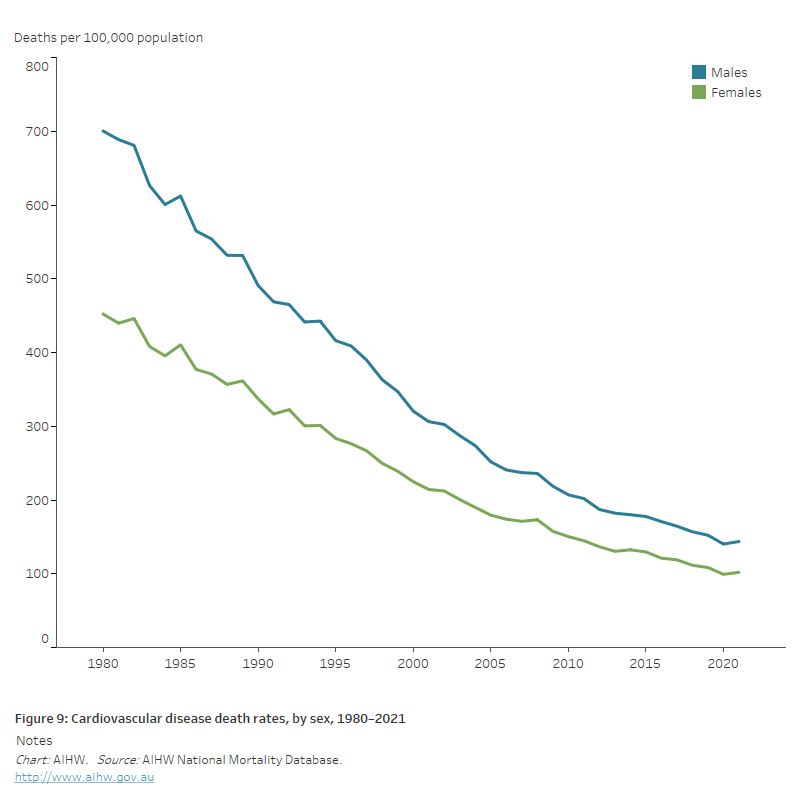
The line chart shows the decline in age-standardised cardiovascular disease death rates between 1980 and 2021, from 700 to 144 per 100,000 population for males and 452 to 102 for females.
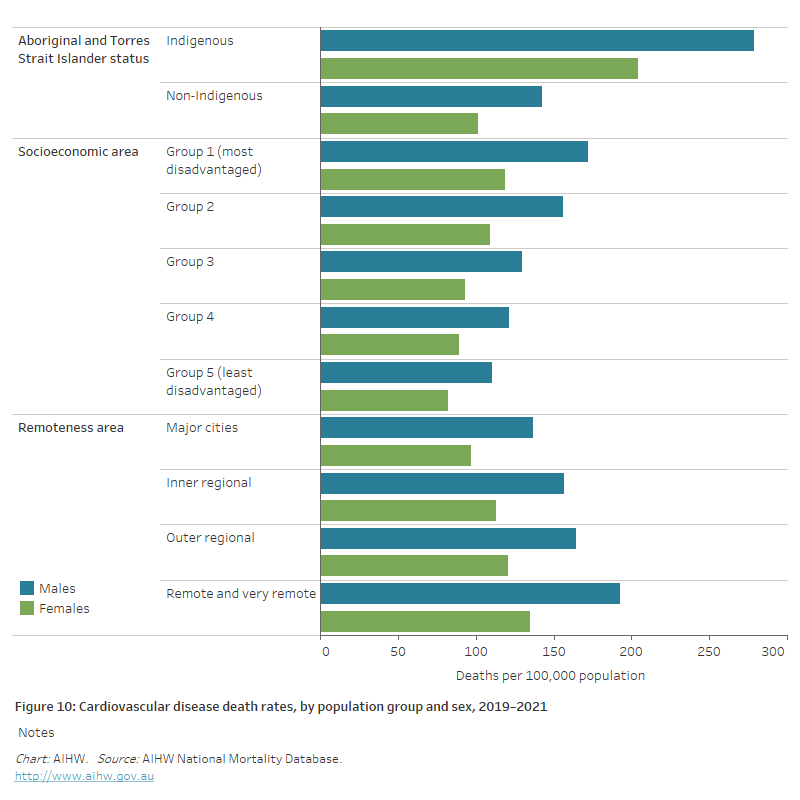
The horizontal bar chart shows that CVD death rates in 2019–2021 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.