How healthy are Australia’s females?
Page highlights
- Self-assessed health status
1 in 2 (55%) of Australian females rate their health as excellent or very good, in 2020–21. - Burden of disease
Females lose more healthy years of life from living with disease and injury (58%) than from dying prematurely (42%). - Chronic conditions
56% of Australian females have 1 or more of the 10 selected chronic conditions. - Cancer
An estimated 73,200 new cancer cases will be diagnosed in females, in 2022. - Mental Health
Almost half (45%) of Australian females have experienced a mental health problem at some point in their lifetime. - Dementia
About 252,000 Australian females aged 30 and over are estimated to be living with dementia, the equivalent of 19.2 per 1,000 females. - Sexual health
Around 62,400 new cases of selected notifiable sexually transmitted infections were reported for Australian females, in 2022. - Reproductive health
- There were around 44,000 endometriosis-related hospitalisations, a rate of 340 hospitalisations per 100,000 females.
- Around 4 in 5 (82%) endometriosis-related hospitalisations were among females aged 15–44 years.
- About 292,000 Australian females gave birth to around 296,000 babies, in 2020.
- Life expectancy and mortality
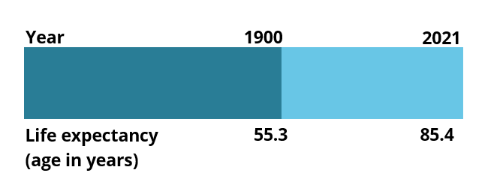
Australian females born in 2019–2021 can expect to live 30 years longer than females born in 1891–1900.
A person’s health status is a general measure combining physical, social, emotional and mental health and wellbeing. A person’s overall level of health can be measured through:
- self-assessment
- burden of disease analysis
- the health impact of disease
- injury in a population
- presence of chronic conditions and comorbidities
- mental health
- sexual health
- life expectancy.
Self-assessed health status
Self-assessed health status reflects a person’s perception of their own health at a particular point in time (ABS 2018b). It can give a broad picture of the population’s overall health (ABS 2018b).
In 2020–21, 55% of females rated their health as excellent or very good. The proportion of females who rate their health as excellent or very good varies by age group. Over two-thirds of females aged 15–24 (69%) rate their health as excellent or very good, compared with 32% of females aged 75 and over (ABS 2022d).
Burden of disease is a measure of the years of healthy life lost from living with, or dying from, disease and injury. The summary measure ‘disability-adjusted life years’ (DALY) measures the years of healthy life lost from premature death (fatal burden) and ill health (non-fatal burden).
In 2022 (AIHW 2022k):
- Australian females experience a smaller share of the total disease burden (47%) than males (53%).
- Females lose more healthy years of life from living with disease and injury (58%) than from dying prematurely (which accounted for the remaining 42%).
- The highest proportion of total burden for females is due to these top 5 disease groups; cancer (16%), musculoskeletal disorders (16%), mental and substance use disorders (12%), cardiovascular (11%), and neurological diseases (10%) (Figure 1).
- Females experience a greater share than males of the total burden from some disease groups including reproductive & maternal conditions (94%), blood & metabolic disorders (which includes iron-deficiency anaemia) (59%), neurological conditions (which includes dementia) (57%), and musculoskeletal conditions (56%).
Figure 1: Leading causes of ill health and death (% DALY) by disease group, females, 2022

Note:
DALY = Disability Adjusted Life–Year. This is a measure of healthy life lost, either through premature death or living with disability due to ill health. It is the basic unit used to measure the burden of a disease.
Source: AIHW analysis of AIHW 2022k
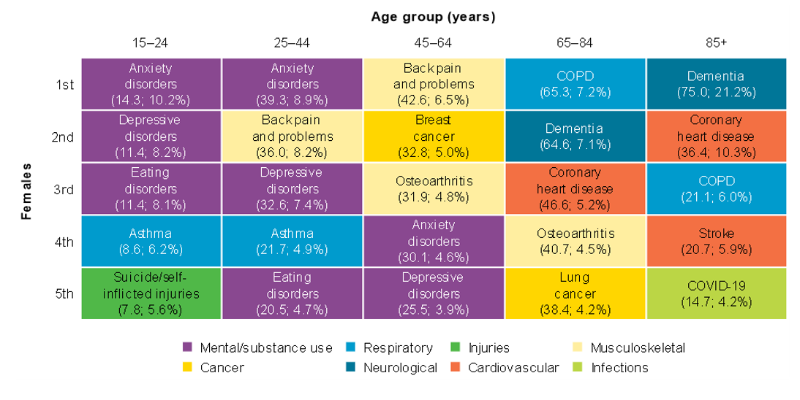
Ill health and death also vary across age groups for females. For females aged 15–44, anxiety disorders are the leading condition. For those aged 45–64, back pain and problems is the leading condition, while for those aged 65 and over, dementia is a leading condition causing the highest ill health (Figure 2).
For more information see Australian Burden of Disease Study 2022.
Figure 2: Leading causes of ill health and death (total burden (DALY’000; proportion) among those aged 15 and over, females, 2022
The figure shows that the incidence of all cancers increases with age, as does the associated mortality. However, mortality is delayed due to the period of living with cancer.

This bar chart shows the rate of dementia across age groups, with the prevalence increasing with age and highest in the oldest age group.

This table shows the number of notifications, per cent of total cases, and age-standardised rates of notifications for chlamydia, gonococcal infection, syphilis, hepatitis b and c for the years 2020 to 2022. For HIV, only 2020 and 2021 data are available.

The line graph shows the notification rates for chlamydia, gonorrhoea and syphilis across the years, from 2012 to 2022. It shows an increase in rates of gonococcal infection and syphilis.

For more information, see HIV, viral hepatitis and sexually transmissible infections in Australia: Annual surveillance report 2022, and the Department of Health and Aged Care National Notifiable Disease Surveillance System.
Reproductive health issues surrounding contraception, unwanted pregnancy, miscarriage, endometriosis, fertility, pregnancy difficulties, menopause and service provision have an impact on economic productivity, quality of life and the physical and mental health of females.
Contraceptive use
Contraceptive choices are complex, and choices made by females may change due to differing circumstances over the life course. A longitudinal study of 17,000 females showed that (Loxton, et al. 2021):
- 60% of females aged 18–23 reported using the contraceptive pill while 45% reported using condoms.
- The use of the oral contraceptive pill decreases from 60% to 34% among females aged 18–23 to those aged 24–29, respectively.
- The use of condoms decreases from 45% to 31% among females aged 18–23 to those aged 24–29, respectively.
- Use of the long-acting reversible contraceptive doubles as females age, increasing from 10% of females aged 28–33 to 24% of those aged 40–45.
- 9% of females aged 18–23 report using no contraception.
Endometriosis
Endometriosis is a chronic condition that can be painful, affect fertility and lead to reduced participation in school, work and sporting activities. Around 1 in 9 (11.1%) females born in 1973–78 are estimated to have been diagnosed with endometriosis by age 40–44 (Rowlands, et al. 2021). Among females born in 1989–1995, around 1 in 15 (6.6%) females are estimated to have been diagnosed with endometriosis by age 25–29 (AIHW 2019b). It takes an average of 5 years for an Australian female to receive a diagnosis after first seeing a doctor (Armour, et al. 2020).
There were around 43,800 endometriosis-related hospitalisations according to the AIHW National Hospital Morbidity Database (NHMD) in 2020–21, a rate of 340 hospitalisations per 100,000 females. Just over half of these (52%) had endometriosis as the principal diagnosis. Around 4 in 5 (82%) endometriosis-related hospitalisations were among females aged 15–44, which are generally regarded as a woman’s reproductive years. This accounts for around 30 out of every 1,000 hospitalisations among females aged 15–44.
Data from the AIHW National Hospital Morbidity Database (NHMD) show rates of endometriosis-related hospitalisations varied by population group, after adjusting for age:
- Females living in Inner regional areas had the highest rate of endometriosis-related hospitalisations (490 per 100,000 females), followed by females living in Major cities (410 per 100,000), Outer regional areas (375 per 100,000) and Remote and very remote areas (265 per 100,000).
- Females living in the highest socioeconomic areas had higher rates of endometriosis-related hospitalisations compared to females in the lowest socioeconomic areas (450 and 335 per 100,000 females, respectively).
- Non-Indigenous females had higher rates of endometriosis-related hospitalisations than Indigenous females (405 and 320 per 100,000 females, respectively).
The reasons for these differences are not known. They could reflect potential variations in access to health services or differences in health-seeking behaviour between population groups, rather than a difference in disease prevalence.
Mothers
An important life stage for many Australians is when they become a parent. For mothers, her health and that of her baby can be affected by a mother’s age, where she lives, the socioeconomic conditions in which she lives, the presence of pre-existing or pregnancy-related medical conditions, and risky behaviours such as smoking and drinking alcohol during pregnancy (Bywood, et al. 2015, UNSW 2022, WHO 2015).
The health and lifestyle behaviours of mothers can have important ongoing implications on both mother and baby. Among Australian females:
- Almost 1 in 10 mothers (9.2%) report smoking at some time during their pregnancy in 2020, a decrease from 14% in 2010 (AIHW 2022j).
- 79% of mothers received antenatal care in the first trimester; 95% had 5 or more care visits (AIHW 2022f).
- Based on pre-pregnancy BMI (calculated based on self-reported height and weight, or measured at first antenatal visit), almost half (48%) of females who gave birth in 2020 were living with overweight or obesity (27% overweight and 22% obese) (AIHW 2022h).
- Most females do not consume alcohol in the first 20 weeks of pregnancy; females are more likely to consume alcohol in the first 20 weeks of pregnancy if they live in Remote (4.6%) or Very remote (9.9%) areas, are Indigenous (8.2%), or are teenage mothers (aged under 20) (4.5%) (AIHW 2022e).
About 292,000 Australian females gave birth to around 296,000 babies in 2020. The rate of females aged 15–44 giving birth was lower than a decade ago (56 per 1,000 females in 2020 compared with 64 per 1,000 in 2010).
The majority of mothers (74%) live in Major cities, 20% of mothers are from the lowest socioeconomic areas, and 36% of mothers are born overseas (AIHW 2022u).
Average maternal age has risen for both first-time mothers (from 30 years in 2010 to 30.9 in 2020) (AIHW 2022g), and those who have given birth previously (from 31.3 years in 2010 to 32 in 2020). The highest proportion of all mothers were aged between 30 and 34 (more than one-third (36%) of all mothers) (AIHW 2022d).
The rate of females giving birth in older age groups has also increased over time. Since 1999 (AIHW 2021h):
- those aged 35–39 giving birth increased by almost 1.5 times, from 47 per 1,000 females in 1999 to 68 per 1,000 females in 2019.
- those aged 40–44 giving birth almost doubled, from 8.4 per 1,000 females in 1999 to 15.5 per 1,000 females in 2019.
- those aged 45–49 giving birth almost quadrupled, from 0.3 per 1,000 females in 1999 to 1.1 per 1,000 females in 2019.
Almost 2 in 3 (63%) mothers had vaginal births, and the remaining 1 in 3 (37%) had caesareans. Caesarean sections were more common among females who were aged 40 and over (56%), and who were overweight (39%) or obese (46%) (AIHW 2022i).
For more information see Mother and babies.
Menopause
During menopause, there are changes to the levels of the hormones, oestrogen and progesterone, and it marks the end of the reproductive years.
The effects of these changes in hormonal levels however, are not just limited to reproduction but can extend to overall health and mental wellbeing. Menopause is associated with an increase in health risk factors and some chronic conditions including (Lancet 2022, Nappi and Simonici 2021):
- cholesterol
- high blood pressure
- overweight and obesity
- coronary heart disease
- diabetes
- osteoporosis
- dementia
- cancer.
Menopause generally occurs at around the age of 50 but can happen earlier.
Certain socio-economic, demographic, lifestyle, reproductive, social, and environmental elements are risk factors associated with premature menopause (earlier than 40 years) and early menopause (40–44 years) (Loxton, et al. 2021). These risk factors include smoking, age at which female had first period, females who experience intimate partner violence and underweight females.
For more information see, Jean Hailes for Women’s Health page on Menopause.
Life expectancy is expressed as either the number of years a newborn baby is expected to live, or the expected years of life remaining for a person at a given age.
This horizontal bar chart shows the leading causes of death in females. Leading causes of death include dementia including Alzheimer's disease, coronary heart disease and cerebrovascular disease.

This horizontal bar chart shows the top three causes of death in rank order, and the changes with increasing age groups. Suicide affects younger age groups most (those aged 15 to 44) but declines in middle age. From age 45 to 74, breast cancer and lung cancer become number 1 ranked causes of deaths. Dementia is ranked number 1 in those aged 75 and over.
