Definitions
Definitions used in reporting maternal deaths
| Type of death | Definition |
|---|---|
| Direct maternal deaths(a) | Those resulting from obstetric complications of the pregnant state (pregnancy, labour and puerperium) from interventions, omissions, incorrect treatment or from a chain of events resulting from any of the above |
| Indirect maternal deaths(a) | Those resulting from previous existing diseases or diseases that developed during pregnancy, and which were not due to a direct obstetric cause, but were aggravated by the physiologic effects of pregnancy |
| Maternal death, not further classified | Deaths considered to be related to the pregnancy or its management, but could not be further classified as either ‘direct’ or ‘indirect’. These deaths are included in the maternal deaths total |
| Coincidental maternal deaths | Deaths from unrelated causes that happen to occur in pregnancy or the puerperium |
| Unclassified death | Maternal death from unspecified or undetermined cause occurring during pregnancy, labour and delivery, or the puerperium |
(a) Definitions are from the International statistical classification of diseases and related health problems, 10th revision, volume 2, section 5.8.1.
Chart: aihw.gov.au
For more definitions of terms used in this report, see the glossary.
Definitions used in reporting perinatal deaths
Various definitions are used for reporting and registering perinatal deaths in Australia. The National Perinatal Mortality Data Collection (NPMDC) collects data and reports using the following definitions:
Figure 1: Definitions of perinatal death
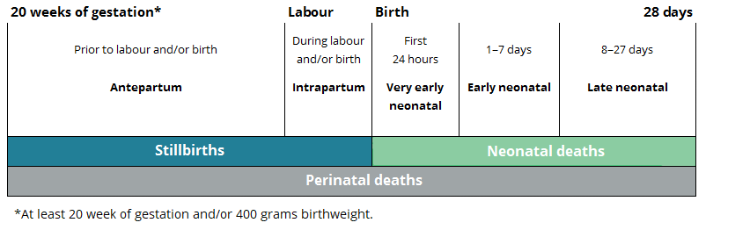
Chart: AIHW
Stillbirth: a fetal death prior to birth of a baby of 20 or more completed weeks of gestation or of 400 grams or more birthweight.
Neonatal death: the death of a live born baby of 20 or more completed weeks of gestation or of 400 grams or more birthweight within 28 days of birth.
Perinatal death: stillbirth or neonatal death of a baby from 20 or more completed weeks of gestation to 28 days following birth or of 400 grams or more birthweight.
Antepartum death: fetal death occurring prior to labour and/or birth.
Intrapartum death: fetal death occurring during labour and/or birth.
Very early neonatal death: death of a live born baby within the first 24 hours after birth.
Early neonatal death: death of a live born within 1–7 days after birth.
Late neonatal death: death of a live born within 8–28 days after birth.
Live birth: the birth of a baby who shows signs of life such as voluntary muscle movement, pulsating of the umbilical cord or presence of a heartbeat at birth, regardless of whether the placenta is still attached or the umbilical cord has been cut.
Terminations of pregnancy: performed at 20 or more weeks of gestation may be included and recorded either as stillbirths or, in the unlikely event of showing evidence of life, as live births. There are variations in legislation regarding termination of pregnancy between states and territories, and recording of terminations is likely to be incomplete.
World Health Organization (WHO) definitions
To allow for international comparisons, the WHO recommendation regarding reporting perinatal mortality, taken from the 2006 Neonatal and perinatal mortality: country, regional and global estimates report has been used. The report recommends publication of rates of fetal death, neonatal death and perinatal mortality of babies weighing 1,000 grams or more, and/or born at 28 weeks’ gestation or more.
This differs from the standard definition used for stillbirths by the WHO, which is the loss of a baby during pregnancy at or after 22 completed weeks of gestation, or if gestational age is not available, with birthweight of 500 grams or more (WHO 2022).
Cause of death classification
The Perinatal Society of Australia and New Zealand (PSANZ) Perinatal Mortality Classification System is used in Australia and New Zealand to classify the causes of stillbirths and neonatal deaths. It includes the PSANZ Perinatal Death Classification (PSANZ-PDC) and PSANZ Neonatal Death Classification (PSANZ-NDC). The PSANZ-PDC system classifies all perinatal deaths by the single most important factor seen as the antecedent cause of death. In addition, for neonatal deaths, the PSANZ-NDC system is used to identify conditions occurring in the neonatal period which resulted in the death.
The PSANZ Perinatal Death Classification is an integral part of the PSANZ Perinatal Mortality Guidelines, developed for optimal standards in investigating, classifying and auditing of perinatal deaths.
From 2019, the National Perinatal Mortality Data Collection (NPMDC) collects data on causes of death that have been classified according to the PSANZ classification system for stillbirths and neonatal deaths, version 4.3 (from 2013–2018, causes of death were in the NPMDC were classified according to the PSANZ Perinatal Mortality Classification System, version 2.2). The classification is recorded as part of each state and territory’s perinatal mortality review process following completion of investigations and at the end of a multi-disciplinary review of the perinatal death.
The other classification system used in Australia to classify perinatal deaths is the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). This classification system is based on the registered cause/s of death on the Medical Certificate of Cause of Perinatal Death, assigned by the treating medical practitioner shortly after death without access to any subsequent investigations.
The National Maternal and Perinatal Mortality Clinical Expert Group (NMPMCEG) (formerly the National Maternal and Perinatal Mortality Advisory Group (NMPMAG)) has concluded that the PSANZ-PDC and PSANZ-NDC classifications are the most appropriate for national reviews. The ICD classification of cause of death has not been included in this report.
PSANZ-PDC primary classification groups
Congenital anomaly: deaths in which a congenital anomaly in the baby (whether structural, functional or chromosomal) is considered to have been of major importance in the cause of the death.
Perinatal infection: primary infections occurring in term and preterm neonatal and fetal deaths and secondary infections in term infants (such as Group B Streptococcus and Cytomegalovirus).
Hypertension: deaths where a hypertensive disorder in the baby’s mother, such as pre-eclampsia or pre-existing high blood pressure, is considered to have led to the death.
Antepartum haemorrhage: all perinatal deaths where the primary factor leading to the death was bleeding from the placental bed in the woman’s uterus.
Maternal conditions: deaths where a medical condition (for example, diabetes) or a surgical condition (for example, appendicitis) or an injury in the mother (including complications or treatment of that condition) is the cause.
Complications of multiple pregnancy: deaths of one or more babies in a multiple pregnancy related to the pregnancy being multiple, including complications of the fetal circulations interconnecting (Twin to twin transfusion syndrome) and umbilical cords becoming entangled where the babies are in only one amniotic sac.
Specific perinatal conditions: deaths of normally formed, appropriately grown babies, in which a specific perinatal condition, such as cord entanglement or a blood group incompatibility, was the main underlying cause.
Hypoxic peripartum deaths: deaths from acute or chronic inadequate oxygen supply from the placenta of normally formed babies, typically of >24 weeks’ gestation or >600 grams birthweight.
Placental dysfunction or causative placental pathology: deaths where the placenta is demonstrated to have been poorly functioning, either by post-mortem microscopic examination of the placental or by ultrasound testing of placental and umbilical artery blood flow.
Spontaneous preterm labour or rupture of membranes: deaths of normally formed, appropriately grown preterm babies following spontaneous onset of preterm labour or spontaneous rupture of membranes, irrespective of whether labour was subsequently induced and mode of delivery.
Unexplained antepartum fetal death: deaths of normally formed fetuses prior to the onset of labour where no predisposing factors are considered likely to have caused the death.
Neonatal death without obstetric antecedent: includes Sudden Infant Death Syndrome (SIDS), postnatally acquired infection (such as Newborn Intensive Care Unit-acquired septicaemia from an intravenous line), accidental asphyxiation and other accidents, poisoning or violence.
PSANZ-NDC primary classification groups
The PSANZ-NDC classification system is applied only to neonatal deaths and classifies them by the most significant condition present in the baby, in the neonatal period, leading to the death.
Congenital anomaly: deaths in which a congenital anomaly in the baby (whether structural, functional or chromosomal) is considered to have been of major importance in the cause of the death.
Periviable infants: neonatal death in infants deemed too immature for resuscitation or continued life support beyond the delivery room (typically infants of gestational age ≤24 weeks or birthweight ≤600 grams).
Cardio-respiratory disorders: neonatal deaths in which a cardio-respiratory condition (such as respiratory distress syndrome or meconium aspiration syndrome) is considered to have been the major contributor to the death.
Infection: neonatal deaths in which infection is considered to have been the major contributor (such as early onset Group B Streptococcus sepsis, pneumonia).
Neurological: neonatal deaths in which asphyxial brain damage (hypoxic ischaemic encephalopathy) or intracranial haemorrhage was considered to have been the major contributor.
Gastrointestinal: primarily includes neonatal deaths related to necrotizing enterocolitis (a medical condition where a portion of the bowel dies).
Other: includes Sudden Infant Death Syndrome (SIDS), multisystem failure, trauma and treatment complications.
References
WHO (World Health Organisation) (2022), International Classification of Diseases for Mortality and Morbidity Statistics, Eleventh Revision (ICD-11), Reference Guide, World Health Organisation, accessed 12 October 2023.