Cervical cancer
Cancer is a group of several hundred diseases in which abnormal cells are not destroyed naturally by the body, but instead multiply and spread out of control. Cancers are distinguished from each other by the specific type of cell involved and by the place in the body in which the disease began.
Cervical cancer affects the cells of the uterine cervix, which is the lower part (or 'neck') of the uterus where it joins the upper end of the vagina (Figure cervical cancer 1). Cervical cancer develops when abnormal cells in the lining of the cervix begin to multiply out of control and form precancerous abnormalities. If undetected, these abnormalities can develop into cervical cancer and spread into the surrounding tissue.
Figure cervical cancer 1: Anatomy of the female reproductive system
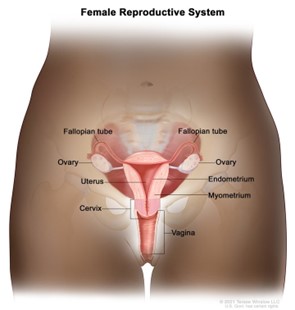
© 2021 Terese Winslow LLC, U.S. Govt. has certain rights
Reproduced with permission of the copyright owner.
Worldwide, cervical cancer is the fourth most common cancer affecting women, ranking fourth for both incidence and mortality; however, its burden is not equal globally. Cervical cancer ranks second in incidence and mortality behind breast cancer in lower Human Development Index countries without cervical screening programs. Cervical cancer incidence is above 25 new cases per 100,000 women in some such countries, compared with a relatively low incidence of 6 new cases per 100,000 women of all ages in Australia (world age-standardised rates) (Bray et al. 2018). This is due to Australia having an organised population-based screening program in place since 1991 that has prevented many cervical cancers by detecting and treating high-grade cervical abnormalities before any possible progression to cervical cancer.
Research performed by the Australian Institute of Health and Welfare (AIHW) using linked cervical screening, cancer, and death data showed that 72% of cervical cancers diagnosed between 2002 and 2012 in women aged 20–69 occurred in those who had either never screened or were lapsed screeners, demonstrating the effectiveness of Australia's cervical screening program in preventing cervical cancer. This research further showed that cervical cancers that did occur in recently screened women were less likely to cause death than those diagnosed in women who had never screened, which is likely due to these cancers being detected at an earlier stage (AIHW 2019).
Human papillomavirus (HPV) plays a major role in the development of precancerous cervical abnormalities and cervical cancer, with HPV being the underlying cause of almost 100% of squamous cell carcinomas and up to 90% of adenocarcinomas (Brotherton et al. 2020) (see Box cervical cancer 1 for further information).
The 4 major steps in most cervical cancer development are:
- infection with HPV (acquired through sexual contact),
- viral persistence (as most HPV infections clear with no treatment),
- progression to precancerous abnormalities (many of which will also regress with no treatment), and
- invasive cervical cancer (Schiffman et al. 2007; Schiffman and Kjaer 2003) (Figure cervical cancer 2).
As indicated by the arrows in Figure cervical cancer 2, the preliminary steps towards the eventual development of cervical cancer are not unidirectional. Most HPV-infected cells return to normal, and a large proportion of precancerous abnormalities do not progress to cervical cancer, even without treatment. However, it is not possible to know which precancerous abnormalities will regress without treatment, and so the detection and treatment of all precancerous abnormalities is important.
While the cell changes caused by persistent infection with oncogenic HPV can cause precancerous changes to the cervix, a range of other factors will influence whether precancerous changes will progress to cervical cancer; these include smoking, multiparity (specifically, more than 5 full-term pregnancies), a young age at first full term pregnancy, oral contraceptive use, and immunosuppression (Cancer Council Australia 2014).
Figure cervical cancer 2: Role of HPV infection in the development of cervical cancer

Source: Reproduced with permission from M Schiffman, National Cancer Institute (Schiffman and Kjaer 2003).
Australia is set to become the first country in the world to actively eliminate cervical cancer, with modelling predicting that the incidence of cervical cancer will drop to fewer than 4 new cases per 100,000 women by 2035, and to fewer than 1 new case per 100,000 women by 2066 (Hall et al. 2019).
Elimination of cervical cancer as a public health problem in Australia
In November 2023, Australia launched its national strategy for the elimination of cervical cancer as a public health problem with a focus on equity. The strategy calls for the delivery of a positive, culturally safe, and inclusive experience of prevention and care, with focus on the following priority populations:
- Aboriginal and Torres Strait Islander people
- Culturally and linguistically diverse people
- People who are LGBTQ+ and people who are intersex
- People with disability
- People living in rural and remote areas
Data are reported annually to assess the progress towards equitable elimination of cervical cancer in the Cervical cancer elimination progress report.
A greater understanding of the role of HPV in most cervical cancers (Box cervical cancer 1) has led to two major developments in Australia, which are behind these anticipated further reductions in the incidence of cervical cancer in Australia. The first of these developments is the introduction of a national HPV vaccination program in April 2007 (Box cervical cancer 2). The second is a renewed national cervical screening program which commenced on 1 December 2017 and uses an HPV test as its primary screening test (Hall et al. 2019).
Note that, while Australia introduced primary prevention of cervical cancer in the form of HPV vaccination that complements the existing cervical screening program, cervical screening remains a vital secondary prevention strategy for those who are HPV-vaccinated and those who are unvaccinated. It is important that all eligible women and people with a cervix participate in cervical screening, irrespective of their HPV vaccination status.
Box cervical cancer 1: Proportion of cervical cancers caused by HPV
It was once thought that all cervical cancers were caused by HPV, but it is now recognised that there are some cervical cancers that are not caused by HPV – the majority of these being some histological types of adenocarcinoma (Hodgson and Park 2019; Stolnicu et al. 2018). Current evidence is consistent with HPV being the underlying cause of almost all squamous cell carcinomas and up to 90% of adenocarcinomas (Brotherton et al. 2020).
In Australia, HPV has been detected in 93% of cervical cancers (Brotherton/Tabrizi et al. 2017). However, the proportion of adenocarcinomas that are present will affect the proportion of cervical cancers that are caused by HPV. The success of cervical screening in reducing the incidence of squamous cell carcinomas has seen the proportion of adenocarcinomas increase in Australia from 11% in 1982 to 26% in 2021. The higher proportion of adenocarcinomas, together with the fact that HPV may no longer be detectable in some cervical cancers caused by HPV (due to loss of HPV DNA over time, for example), has contributed to HPV being detected in 93% of cervical cancers in Australia.
In the future, it is likely that the proportion of cervical cancers in which HPV is detected will fall. This would be an indication of a successful cervical screening program, with further reductions in the cervical cancers that are caused by HPV leading to a higher proportion of cervical cancers that are not caused by HPV (Brotherton et al. 2020).
Box cervical cancer 2: HPV vaccination in Australia
In April 2007, Australia introduced the National HPV Vaccination Program, which included an ongoing program for girls aged 12–13 and a 'catch-up' program for girls and women aged 14–26 through to the end of 2009. This program was extended to boys from February 2013. The HPV vaccine is now administered to girls and boys aged 12–13 years at school under the National Immunisation Program (NIP).
In 2018, Australia commenced using the nonavalent HPV vaccine Gardasil9 protecting against an additional 5 types of HPV, replacing the quadrivalent vaccine Gardasil. The number of doses required was reduced from 3 to 2.
Gardasil9 protects against types 6, 11, 16, 18, 31, 33, 45, 52, and 58 compared with Gardasil that protected against types 6, 11, 16, and 18. This vaccine will further improve the protection against women developing cervical abnormalities and cervical cancer.
In 2023, Australia reduced the number of HPV vaccine doses required to just a single dose, based on strong evidence of protection from a single dose. NIP-funded single dose catch-up HPV vaccination is now available to all people aged up to and including 25 years.